
Jan 11, 2021 | Medical Billing Customer Service, Medical Billing Software Blog, Medical Billing Software Customer Service, MIPS Reporting, Revenue
It goes without saying that 2020 will go down in the history books as unprecedented for us at EZClaim. Still, we worked hard to stay positive and navigate the storm by offering resources to you, our clients, the content that matters to you. As an end-of-year bonus, and a ‘kick-off’ for 2021, we reviewed the blogs and social posts you read and reacted to the most and thought we would share them.
So, here are the best blog posts of 2020:
#1: How to Improve Medical Billing Revenues
As a medical billing company, we work hard to understand how we can help our clients increase their revenue and improve their billing process. Those who do this best are experts in the medical billing and coding industry. So, it makes complete sense that your interest peaked on our article concerning improving revenues. Enjoy reviewing our number one article of 2020! [ Click to read the post ].
#2: What Will Be New for E/M Coding in 2021?
Last year brought about a long list of changes to billing and coding, as well as, the medical industry as a whole. From the obvious boom in Telehealth, to the updates in evaluation and management services, those working in the industry were impacted immensely. Based on these shifts in industry and the impact on you, our clients, we thought a look into what was coming in 2021 would be useful—and so did you. You read, reacted, and shared the value of this content with others. Now we are sending you a reminder that this was our number two article for the year. [ Click to read the post ].
#3: Collecting Payments from Patients. Find Out How.
No matter how chaotic things get, there is still a practical side of our industry that needs to be addressed. That is why we worked to keep the focus on the basics, speaking about the ‘bread and butter’ of our industry, collections. In this practical article, we focused on the keys to educating the patient and how doing so will help keep you ahead of the collection as a whole. [ Click to read the post ].
#4: Reports – Nuisance or Necessity?
At the end of the day, you want to go home and no one wants to be stuck in the office doing double-duty on reports. You know as well as we, that getting reports done correctly the first time is key to reducing stress and going home happy. That is why we distilled some of the keys in running reports that would make your life more straightforward. The fourth article on our list will do just that by helping you make sure the dates, details, and destination of your reports are in the right place. [ Click to read the post ].
#5: Why Do I Have A Balance? – Patient Payments
Saving the best for last, especially as we approach tax season, we come in with our final of our best of 2020 by talking about balances. Every practice ends up spending those final hours of the year figuring out where those dollars and cents went. In this article, we gave you tips on deductibles, co-pays, and max out-of-pocket that helps your bottom line. Closing out 2020, don’t miss a few keys to help you balance the books. [ Click to read the post ].
These are EZClaim’s best blog posts of 2020, but these were not the only blog posts we did. So, if you would like to explore the other blog posts we did, click here for our blog page.
————————-
ABOUT EZCLAIM:
EZClaim is a medical billing and scheduling software company that provides a best-in-class product, with correspondingly exceptional service and support. Combined, they help improve medical billing revenues. To learn more, visit EZClaim’s website, e-mail support, or call a sales representative today at 877.650.0904.
Jan 11, 2021 | Electronic Billing, Health eFilings, Medical Billing Software Blog, Partner
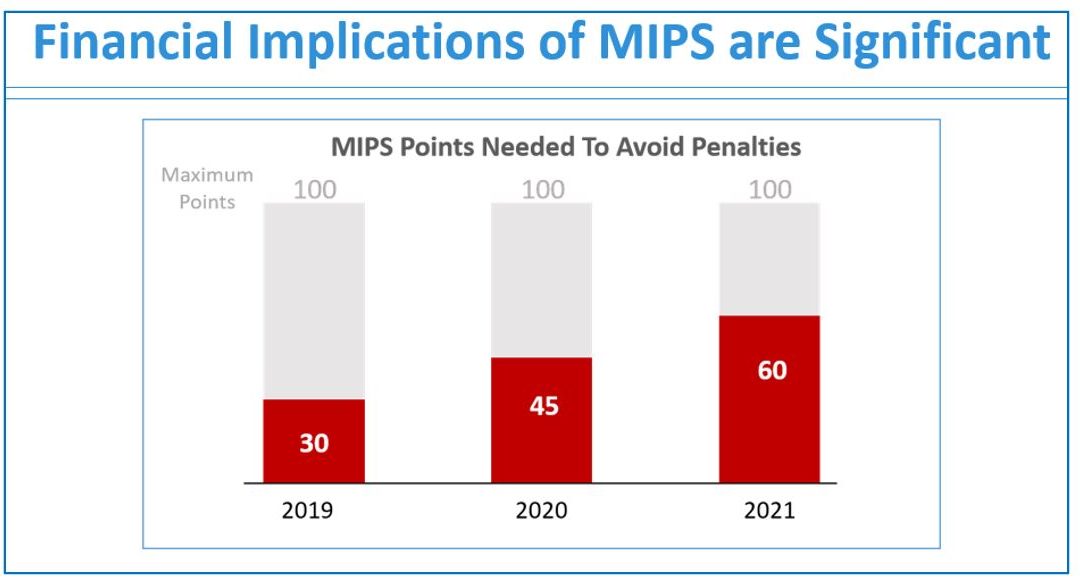
If you are not a MIPS expert (Merit-based Incentive System), your Medicare reimbursements may be decreased by 9% in the next year. However, it’s not too late to avoid the penalty for the 2020 reporting period, but you need to act now!
One of EZClaim’s partners, Health eFilings’ has ONC-certified software that completely automates the MIPS compliance process for you. The software will automatically extract the required data directly from EZClaim (and/or your EHR), and then proprietary algorithms will process the 9,000,000 possible combinations of quality measures for each clinician to identify which measures should be submitted to CMS (Centers for Medicare and Medicaid Services) to earn you the most points.
Need a MIPS expert? Well, Health eFilings is one of the best, and CMS has accepted 100% of their submissions on behalf of their clients. If you have completed your 2020 reporting, reach out to them, and learn how you can earn even more points in 2021.
For more information about EZClaim’s medical billing software, e-mail, visit their website, or contact them at 877.650.0904.
[ Article contributed by Sarah Reiter, SVP Strategic Partnerships, Health eFilings]

Jan 11, 2021 | BillFlash, Medical Billing Software Blog, NexTrust, Partner
There are five primary medical practice fundamentals that, if focused on, will ensure your practice is working toward goals that will make the biggest difference. Practices are pulled in many directions each day, and it can be difficult to know what to prioritize, so the following are some recommendations.
1) Define Patient Engagement Goals
Perhaps one of the most overused terms in today’s medical field is “patient engagement.” Much like the drawer filled with important yet miscellaneous items, if you can’t actually define it, you probably aren’t going to do something with it.
In 2021, it is imperative to define your office’s patient engagement goals in order to determine whether they are being met, and more importantly, if the value you’ve placed on engagement is benefitting your bottom line. This could include engaging via a more personal checkout process that explains how billing and payment will be done and asking patients if there are certain times of the year they wish to be notified for annual wellness checks.
2) Ask For Online Reviews
Reviews remain one of the highest drivers of new customer acquisition. As a local business, you can create a Google Business account online that provides your address, phone number, and link to your website. Included is the ability to add reviews as well as phrases and keywords about your business within the Google Business dashboard, and it’s all free!
To encourage your patients to leave reviews, create cards with step-by-step instructions for posting online reviews via Google. Be picky. Make sure you ask your best patients to participate, who will be honored that you asked. Don’t forget to monitor to see how your business listing looks to potential new patients.
3) Offer Friendly Medical Bills
Of course, we’re not suggesting you add flowers or poignant sayings. Rather, explain a statement to your patients at checkout or within their financial package; this helps the process flow more naturally. BillFlash patient statements have five different messaging rows you can customize for communication. Plus, you can also send electronic patient statements through text and email.
In 2021, communication with patients—even on billing statements—should be natural, friendly, and simple. Getting paid is a segment of the medical practice workflow and should be as easy and frictionless as possible.
4) Ask About Payment Preferences
People are driven by routine and behavior. In today’s world, when paying for an item, the buyer is offered numerous options including cash, debit and credit, no-interest, pay-over-time plans, payment apps, or even Near Field Communication (NFC) like Apple and Google Pay. Granted, the last two have had very low adoption rates, but keeping an eye on payment trends costs little more than time and may add something unexpected to your bottom line.
In 2021, identifying the preferred patient payment options could be the difference between getting paid quickly and not getting paid at all. Don’t overlook the enormous value people place on how they give and take money.
5) Use RCM Services
An RCM vendor helps you get the most out of your practice revenue. They help you collect more from difficult balances, empower patients to pay in full, and improve your claims processing—without adding extra work for your office staff. Working with the right RCM services provider ensures you are paid more for the work you do. They also help identify reasons for claims denials, which have a positive impact on your practice revenue, as well.
For more information about automated patient statements and patient payment options, contact EZClaim, NexTrust BillFlash, GetPaid@BillFlash.com, or call BillFlash at 435.940.9123 (Option 3). For more details about EZClaim’s medical billing software, visit their website, e-mail their support team, or call them at 877.650.0904.

Jan 11, 2021 | Electronic Billing, Medical Billing Software Blog, Partner, Trizetto Partner Solutions
With a new year comes new medical coding changes.
After the examinations, x-rays, and surgeries, lives another major part of a physician’s day that happens behind the scenes. All the hard work needs to be processed through a successful claim submission, meaning that ultimately earning payment all boils down to one thing – coding. Evaluation and management codes, or E/M codes, are codes a physician uses to report a patient visit. This administrative task – a necessity for any physician – is often cumbersome and prone to errors. Most importantly, it uses up valuable time that could be better spent.
How many of us have experienced the “hurry up and wait” scenario? The type of appointment where you wait in a waiting room, then wait a little more in the exam room, then eventually get 10 minutes with your doctor…only to be rushed out so the next patient can be shuttled in. Unfortunately, it’s all too common. It’s safe to say that many patients could benefit from more face-to-face interaction with their providers.
Many people claim that payment for evaluation and management services is undervalued, specifically when it comes to ambulatory services. Additionally, it’s been argued that the fee schedule itself is not well-designed to support primary care, which requires ongoing care coordination for patients. Pressure existed to increase payment rates for ambulatory E/M services while reducing payment rates for other services. Thankfully, The Centers for Medicare and Medicaid Services (CMS) took notice. With the goal of increasing efficiencies to reduce unnecessary burdens, the “Patients over Paperwork” initiative was established. Per CMS, E/M codes make up 20% of total spending under the physician fee schedule. Part of this initiative aims to reduce the coding and documentation requirements for E/M codes, in turn giving physicians more time to spend with patients. In partnership with The American Medical Society (AMA), CMS worked to revise the rules for evaluation and management coding requirements. These changes were finalized in the 2020 Physician Fee Schedule (PFS) with an effective date of January 1, 2021.
So what exactly was revised? The E/M updates affect codes 99201 through 99215 and include the deletion of code 99201 along with revisions to the code selection for 99202 – 99215. Below is a summary of the revisions to E/M codes:
- Elimination of code 99201
- Decrease the burden of coding requirements
- Decreases the burden of documentation
- Decreases the need for audits
- Revises the definitions for Medical Decision Making (MDM)
- Revises the definition of time spent with the patient to total time including non-face-to-face for E/M services by a physician and other QHP
- Requires a history and/or examination when medically< necessary
- Offers a clear time ranges for each code for time spent with the patient
- Addition of a new 15-minute prolonged service code
- Clinicians will choose a code based on MDM or total time
These changes apply to office visits and other outpatient services. It’s noteworthy that these changes represent the first changes to the E/M codes in over 25 years! More importantly, the changes streamline the coding process, reduce clinician burden, and will allow physicians to put the focus back on patient care.
Billing and coding should always be top of mind, but it can be hard to keep up. This is why it’s critical for physicians, clinicians, coders, and billers to completely understand these changes. To help comprehension, the AMA released a checklist identifying ten steps to help the practices prepare for the upcoming changes that can be accessed here. To learn more about the medical coding changes and the summary of revisions, visit the AMA website.
TriZetto Provider Solutions is a partner of EZClaim, and can assist you with all your coding needs. For more details about the EZClaim medical billing solution, visit their website, e-mail their support team, or call them at 877.650.0904.
———————–
Note: This article is not a comprehensive overview and is NOT intended to provide coding advice, rather it is intended to highlight the new changes in effect and the need for physicians to ensure they have received the proper training for the upcoming changes.
[ Contributed by TriZetto Provider Solutions Editorial Team ]

Dec 14, 2020 | Live Compliance, Medical Billing Software Blog, Partner, Support and Training
There are a few HIPAA items to focus on RIGHT NOW—before the end of 2020!
The U.S. Department of Health and Human Services (HHS) has designated the “Health Insurance Portability and Accountability Act” (HIPAA) as the national standard for protecting the privacy and security of health information (in 1996). This led to the Health Information Technology for Economic and Clinical Health Act (HITECH), which has a provision in it for audits, and the HHS Office for Civil Rights is responsible for carrying out HIPAA audits, and responding to complaints and breaches. Ignoring them is not an option!
A Risk Assessment IS NOT Enough
A risk assessment is only one element of the compliance process. You must also “implement security updates as necessary and correct identified security deficiencies.” In other words, you must act via a Corrective Action Plan (CAP) and follow the required risk assessment process.
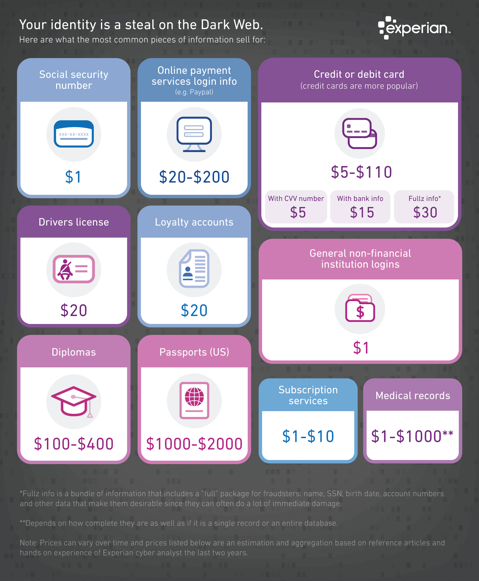
Dark Web
It is no secret that the “Dark Web” is a scary place to lose your information. So, what if it did happen and affected your entire company? Identity thieves get anywhere from $1-$1,000 for medical records, for each instance! So, how can you protect yourself and/or your organization?
Well, data breaches are becoming more common—sometimes which are out of your control—so carefully monitoring where you store and enter your passwords can be extremely beneficial to help minimize the risk of a hack and keeping personal or patient information protected.
One solution for this is the automatic Dark Web monitoring built into the portal of one of EZClaim’s partners, Live Compliance. Their solution helps keep an ‘eye’ on employees whose information was involved in a breach, and suggests next steps to take where the breach was found. Then, it allows your to conduct an accurate and thorough Security Risk Assessment. This is not only required, but is a useful tool to expose potential vulnerabilities, including those that involve password protection.
 So, what can I do to ensure this doesn’t happen to me or my organization? Well, Live Compliance makes checking off your compliance requirements extremely simple by providing:
So, what can I do to ensure this doesn’t happen to me or my organization? Well, Live Compliance makes checking off your compliance requirements extremely simple by providing:
● Reliable and effective compliance
● Completely online, our role-based courses make training easy for remote or in-office employees
● Contact-free, accurate Security Risk Assessments are conducted remotely. All devices are thoroughly analyzed regardless of location.
● Policies and procedures are curated to fit your organization, ensuring employees are updated on all workstation use and security safeguards in the office, or out. It is updated in real time.
● An electronic document is sent to employees and business associates
So, don’t risk your company’s future, especially when Live Compliance offers a FREE Organization Assessment to help determine your company’s status.
For additional details, call them at 980.999.1585, e-mail them, or visit their website at LiveCompliance.com
[ Article provided by Jim Johnson of Live Compliance ].
ABOUT EZCLAIM:
EZClaim is a medical billing and scheduling software company that provides a best-in-class product, with correspondingly exceptional service and support. Combined, they help improve medical billing revenues. To learn more, visit EZClaim’s website, e-mail them, or call a representative today at 877.650.0904.

Dec 14, 2020 | BillFlash, Medical Billing Software Blog, Partner
If your New Year’s resolution is to get your practice back into tip-top shape, now is the time to determine your best ‘recipe’ for billing and payment success. In the spirit of the holidays, where award-winning recipes are part of the season, we have included our proven ‘recipe’ for billing and payment success:
INGREDIENTS:
– EZClaim billing software
– Patient statements
– Text & email eBills
– Online payments
– Payment plans
– Stored payments
– Automated payments
– Integrated Collection Services
PREPARATION:
Begin with EZClaim practice management software. Add integrated patient statements, and the ability to text and e-mail eBills. Then, mix in online payments, payment plans, automatic payments, and stored payments. Bake for 30-90 days, and watch your revenue rise! If needed, add a ‘dash’ of Integrated Collection Services to increase your serving amount.
Shape your billing and payment success by adding Pay Services, which will help your practice thrive financially in the new year (More details in this 60-second video). Also, view the Integrated Collection Services Video to learn how you can begin automating and simplifying the patient collections process.
OK, you might have found that a creative use of ‘recipe’, but you probably really want to see the Gingerbread cookie recipe in the photo. So, here it is:
Ingredients:
– 1/2 cups softened butter
– 1/4 cup packed brown sugar
– 1/4 cup granulated sugar
– 1 large egg
– 2 teaspoons ground cinnamon
– 1 tablespoon ground ginger
– 2-1/4 cups of flour
– 1/2 cup molasses
– 1 ‘dash’ of love
Preparation:
Cream butter and brown sugar together. Stir in molasses, then the egg. In a separate bowl, mix flour with all the spices. Stir in butter/sugar mix. If dough is too moist, add 2 tablespoons of flour.
Knead dough lightly, then chill for 40 minutes. Shape the dough into desired shapes. Bake at 350F until tops are ‘set’ (abut 8-12 minutes). Cool on a wire rack for at least 2 minutes before indulging! (If you don’t eat them all in one ‘sitting’, store them in an airtight container, at room temperature, for up to one month!).
[ Click here to download this delicious Gingerbread cookie recipe. (Also, we would love to see pics of your decorated cookies. Send them to sales@ezclaim.com) ].
As we approach the holiday season, EZClaim hopes that you are able to enjoy this time with your families!
ABOUT EZCLAIM:
EZClaim is a medical billing and scheduling software company that provides a best-in-class product, with correspondingly exceptional service and support. Combined, they help improve medical billing revenues. To learn more, visit EZClaim’s website, e-mail them, or call a representative today at 877.650.0904.